
|
I have been pretty consistent over the years in several regards. I begin most days running trails or training, I am an early riser, a voracious reader, and I have no idea what clients think they are measuring when they ask about "race" either in survey demographics or as a dimension in analysis. As a recovering bench scientist, I am aware that groupings by race show less inter-group variability genetically than inter-personal differences within the population at large. Basically it means we are all the same. Race science has been debunked since World War II although there is a group of avid scientists that got the memo but either aren't reading it or have too much to lose if they did. I have read about different rates of hypertension in black cohorts for example but we aren't offering meaningful biologic causes--and why do these differences disappear in African countries? It would appear we have home grown factors here that bear examination. Instead of creating arbitrary cohorts based solely on "race" shouldn't we ask if oxidative stress differences might be attributed to other social and political factors? How is this possible if we rely on underpowered check-box mentality towards race? The centuries-old belief in racial differences in physiology has continued to mask the brutal effects of discrimination and structural inequities, instead placing blame on individuals and their communities for statistically poor health outcomes.  Although 1619 leaves many gobsmacked regarding the roots of slavery in the United States--the actual date is even earlier. "The Spanish took enslaved Africans to a settlement in the present-day Carolinas in 1526. The slaves rebelled, and the settlement failed. Also, the Spanish took African slaves to St. Augustine, Fla. — which, unlike the Jamestown colony in Virginia, still thrives — in 1565--Rex Springston, Virginia Mercury If only for historical curiosity, these stories from the New York Times are timely and at the same time quite overdue. My initial quest began when I had to figure out what to do with the data. Race is a poor biologic proxy because it is and has always been a social or political construct. As an analyst I either need the social construct you seek to measure or I need the actual biologic entity you seek to evaluate--just collecting race is useless. I can do a little bit if we capture ancestry as we anticipate genetic drift to be associated with geographical origins but again, in the absence of a well-formulated question or hypothesis it isn't as relevant as you might think. A recent article in JAMA Oncology wields race into a surprisingly quotidian narrative. The argument seems to be we need to improve recruitment of minorities into clinical trials but falls apart when there isn't really a compelling data infrastructure for yielding meaningful insights if this goal was achieved. Are we measuring the right things or just data mining for signals? For trials that did report on race, there were notable disparities in the makeup of participants. White patients accounted for 76% of study participants, while Asian patients accounted for 18%. What exactly is a black patient? Is the presence of identification as black even relevant? Think of the diversity or stories of origin of this deeply heterogeneous population. Would findings from someone from Ghana be able to be extrapolated to individuals from say Somalia? Is the perceived appropriateness and political correctness of African American as a descriptor clouding our short sightedness of grouping every "other" according to the melanin in their skin or other phenotypic characteristics? It is unreasonable to assume that classifying individuals based on an entire continent of origin would yield granularity needed to answer a data question or hypothesis. Disparity of Race Reporting and Representation in Clinical Trials Leading to Cancer Drug Approvals From 2008 to 2018--link to article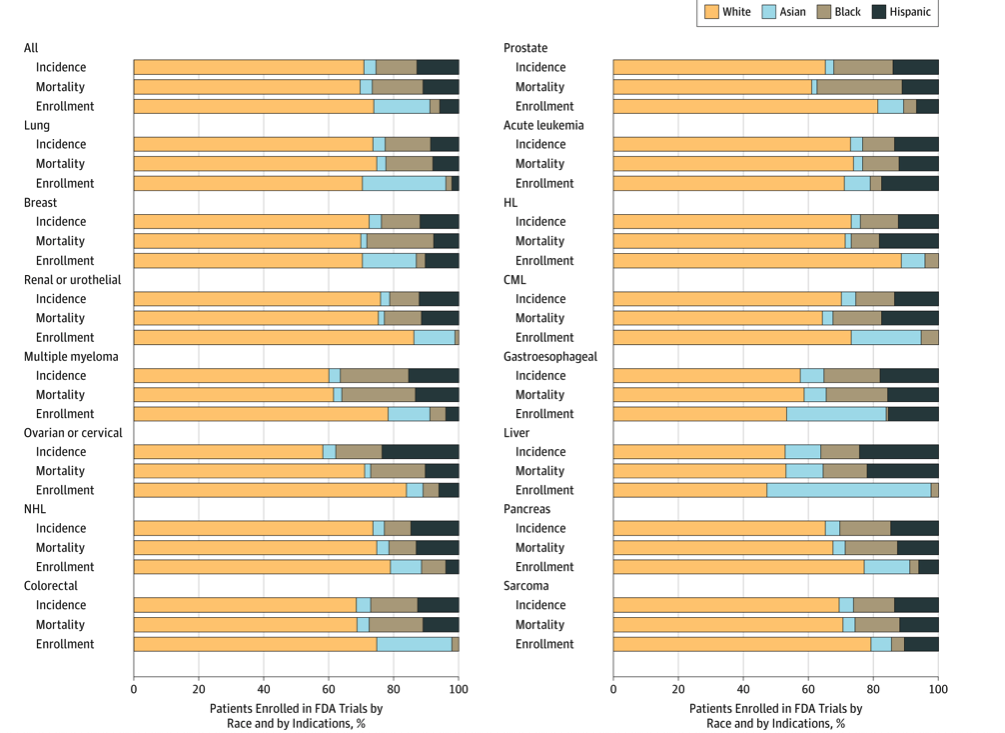 The JAMA article does mention (right before the conclusions) "We also recognize that social, economic, and environmental factors are equally important factors in propagating disparities in cancer care." If equally important, we need to be having those discussions and selecting additional variables to capture these factors and include them in analyses. One final thought, the elephant in the room is the lack of upstream research and funding into the multi-pronged causative factors of cancer. The research describes water toxicity, poor air quality, stress in general, inadequate nutrition, low education, access to care, inadequate livable housing, influence of agri-business, and a myriad of societal and economic drivers of low health. How would these 4 racial groups rank on exposure to these known social correlates of health and disease? Is this an opportunity for medical intervention or societal and political reform as prevention? Courtesies of a small and trivial character are the ones which strike deepest in the grateful and appreciating heart--Henry Clay  Comments are closed.
|
