

Darwin's theory of evolution is a framework by which we understand the diversity of life on Earth. But there is no equation sitting there in Darwin's 'Origin of Species' that you apply and say, 'What is this species going to look like in 100 years or 1,000 years?' Biology isn't there yet with that kind of predictive precision.--Neil deGrasse Tyson
Our precise understanding of the complex biology behind cancer immuno-oncology lags the reported outcomes observed in clinical research. Case in point--the best therapies on average confirm clinical trial endpoints in approximately 20 to 30 percent of patient populations. I would argue that we are measuring the wrong thing but more about that later.
In the last 6 months to a year I have been working almost exclusively in the immuno-oncology space. Either directly with industry, on a collaborative team, or as a numeracy expert helping physician groups and/or patient advocacy groups unpack the latest findings. After attending the World Vaccine Congress, Immunology 2017, DIA/FDA Statistics Forum, and Duke-Margolis Center for Health Policy/FDA workshop on analytical validation of assays used in qualifications of biomarkers I can tell you the headlines announcing potential cures and breakthrough approvals for checkpoint inhibitors are misleading and superficial in their conveyed messages. Here is a simplistic representation of immunotherapy to introduce you to the basic premise in case this isn't an area of expertise.
The Cure in the Code: How 20th Century Law is Undermining 21st Century Medicine by Peter W. Huber describes the historical precedence and evolving shift of a small molecule mind-set to the rise of biomedical science and the power of a data-enabled framework. The first-pill costs are markedly more expensive than the later-pill costs--the true excipient is the "know-how". Are we ready to rethink our mindset? How do we market knowledge?
What if we approved drugs based on the biochemistry. Similar to Eureresist what if drugs were classified based on their ability to increase trafficking and penetration of tumor by T cells, T cell activation, and quantity of tumor-specific T cells for example. We can look at the graphic and see the myriad of options. What may result is the combination of HIV style cocktails that tailor treatment to the specific biochemistry of the tumor AND the patient. In the absence of clunky monotherapy or combination therapies we don't truly understand--we now have measurable endpoints beyond overall survival, progression free survival, etc. 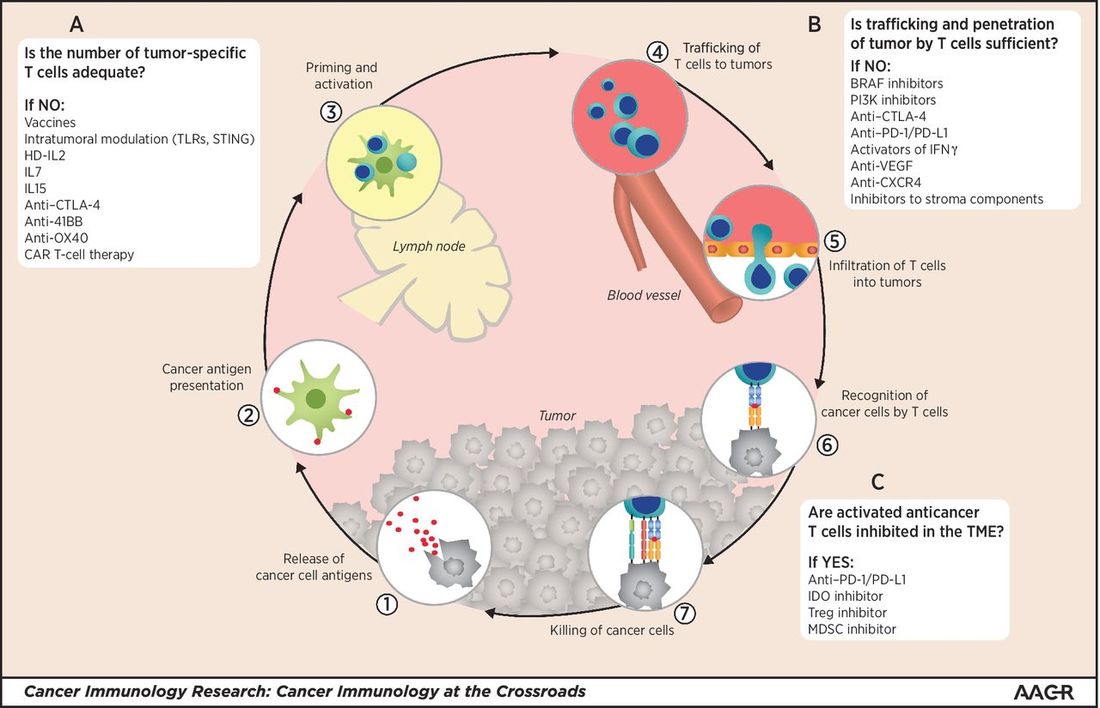
Why is the latest data from Keytruda heralded as the success of ASCO while Opdivo, once the industry leader is losing it's footing with less than impressive two-year survival update on its Opdivo-Yervoy first-line lung cancer? I am going to point to the complexity of identifying appropriate biomarkers.
The most-effective to date has been PD-L1 expression but we shouldn't be convinced of a simplistic one biomarker gateway. An article published in 2016 by Manson and colleagues Biomarkers associated with checkpoint inhibitors highlight biomarkers with the potential to predict efficacy and toxicity. 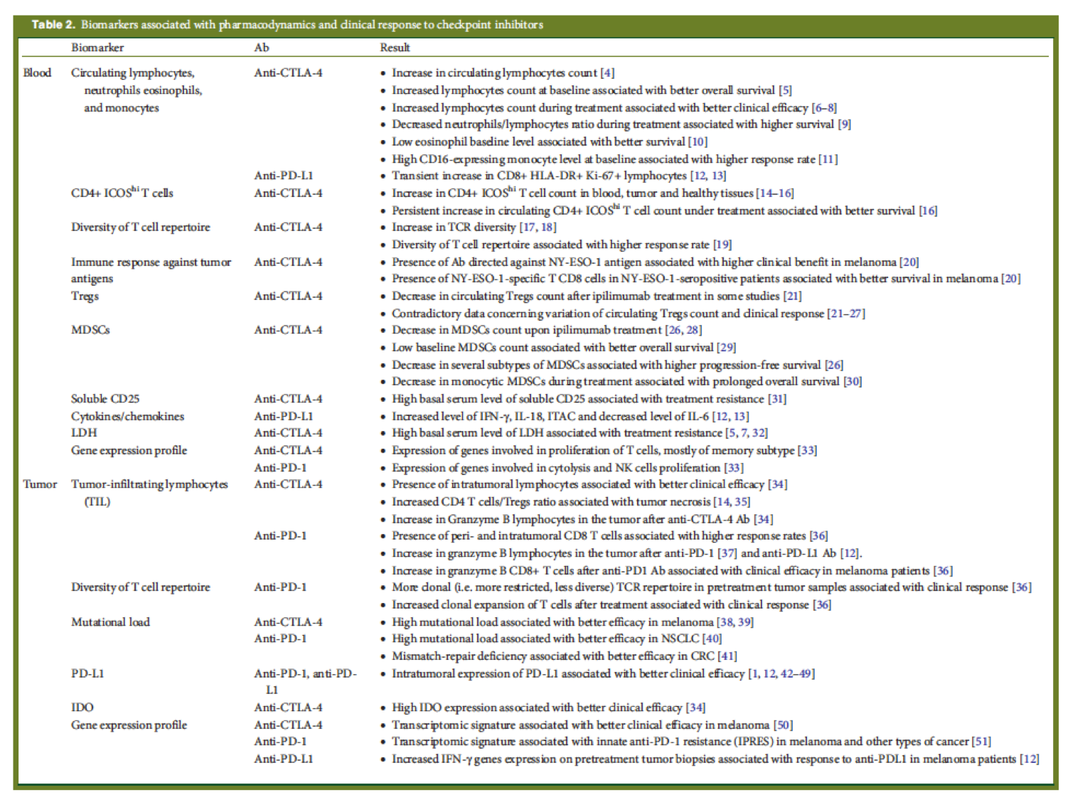
The Biomarker Assay Collaborative Evidentiary Considerations Writing Group, Critical Path Institute (C-Path) includes scientists from the FDA, industry and academia collaborating to establish scientific and regulatory validation of biomarker assays. The process is ongoing and complex and includes a "framework" approach vs. a "checklist" to help stakeholders quantify and validate their assays effectively.
Inherent in the measurement of biomarkers, unlike the measurement of xenobiotics (drugs), is that biomarkers are endogenous entities or molecules. Therefore, biomarker assays typically measure an increase or decrease in the endogenous level of the molecule which often fluctuates because of individual variability in physiology, disease biology, pathology, comorbidities, treatment administered, and environmental factors. Given these factors, the requirements and expectations for assays used in the qualification of biomarkers must take into consideration 1) the type of molecules being measured and 2) the context in which the biomarker is being applied in drug development and in regulatory decision-making.--Public Workshop Duke Margolis Center for Health Policy, DC 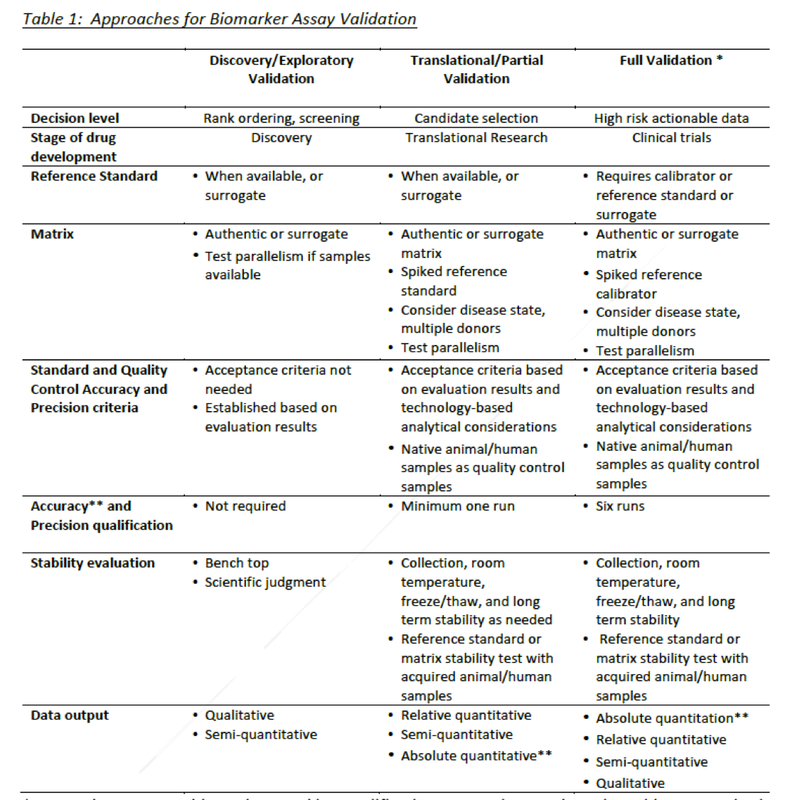
The new prescription for medicine might indeed be ex uno plura--out of one, many--an evolution from epidemiology and crowd-sourced aggregated solutions to single-gene perspectives and truly tailored treatment for the unique biochemistry of an individual.
There is a lot of crowd speak about reforming how we develop drugs--especially in the US. Don't get me wrong, I listened carefully during the DIA/FDA Statistics Forum about adaptive frameworks, pragmatic trials, how to analyze real world evidence and integrate findings with clinical trial data generated from well-defined, perhaps ineffectual, clinical endpoints. There also seems to be an inexhaustible variety of innovative strategies being circulated to manage the ginormous data deluge and focus on patient driven outcomes. As a writer coming of age both personally and professionally during the early years of the HIV crisis I remain curious about our relative amnesia or short attention spans for the hard-won lessons learned during a pivotal time in clinical science. The most powerful patient advocacy in the world drove the positive outcomes and clinical successes most of us take for granted. The leading edge of the science existed at the front line--well before long-term outcomes in efficacy and safety were established. I don't want to ruin your morning but dear reader, "safety" is not even a scientific term. Because of the "interesting" evolution of the Food And Drug Administration (FDA)--and you definitely should read up on how we landed where we are today--and how gaps persist where real science can occur (The Cure in The Code: How 20th Century Law is Undermining 21st Century Medicine)--we are forgetting, at our own detriment, how off-label prescribing, critical thinking, and physician/clinical scientist group-think led to Euresist. The development of an international computer-based clinical management of antiretroviral drug resistance informed providers about what to do if a patient's viral load--once suppressed--escalated. What therapy or cocktail has proven effective?
The physicians were prescribing drugs effective in leprosy to patients with aggressive fungal disorders, wasting syndromes, and oral and genital canker sores characteristic of AIDS--not because they were FDA approved--but because they worked. The evolution of EuResist provided a tool for physicians to make evidence-based decisions (even if evidence was still evolving at the clinical level) at the point of care outside the government process that had proven to cumbersome to respond to the scale of morbidity and mortality. EuResist Network is a partnership of eighteen institutions in Europe and beyond, which promotes and coordinates joint research and dissemination efforts of its partners. As my inbox "pings" with late breaking news of ASCO data and invitations to webcasts I think we are witnessing the pivot from compassion and improving patient outcomes to expanding market share and market driven profits. I am not tossing babies out with volumes of bathwater--but seriously--where is the framework for a free open-sourced group think? I know there are pockets of sharing. I have written about them here. The model of for-profit data outpaces the network open-source solutions. Huge databases are amassed with partnerships boasting genetic libraries, claims data, clinical trial data and real world data--for a fee. A whopping fee with no promise of relevance or operational insights. What is the solution? Provide context and conceptual understanding so healthcare providers can group-think knowing they have actionable data. An ever increasing number of immune-oncology (I/O) therapies are being granted break-through designations. I am excited to hear the latest data from larotrectinib, a novel selective TRK tyrosine kinase inhibitor (TKI). The high response rate is intriguing. Those of us lucky enough to be present in science have a responsibility. Not to repeat sensationalized headlines but to help unpack the data in an industry agnostic manner. What do findings mean? Real world data is generated one patient at a time. It is up to us to assess real world evidence and share the narrative. It will be the providers at the point of care evaluating tumor genetics, micro-environments, mutational attributes of exomes, neoantigens, cell-cell signals of kinase pathways, and more as 'n of 1' findings outnumber epidemiological population estimations. Despite durable responses to TRK kinase-directed therapy in patients with NTRK-rearranged A sentence in The Cure in the Code has stayed with me, "A drug can be judged unfit for the market, one arm of government limits what the drug company may say while another invites juries to read lies or broken promises into its silence-Peter Huber
Stay-tuned for findings from the LOXO webcast scheduled June 4th... |


