
A few simple truths...For screening to prevent people from dying early, simply finding cancers is not enough; we need to find progressive cancers that would kill if left untreated. What’s more, we need effective treatment for these cancers. And the therapy has to be more likely to cure if administered earlier (when cancer may be detected by screening) than later (when cancer may be detected by the patient or doctor without screening).--When Talking about Cancer Screening, Survival Rates Mislead 
To detect cancerous cell types upstream from actual disease and then attribute it as an advancement of 5-year survival has little or no impact on overall mortality. Lead time bias advances the diagnosis by comprehensive screening but isn't likely to impact mortality rates. As you can see, if we improve detection of a cancer that is slow growing to begin with or indolent and not likely to progress--we can't say that screening improves mortality rates.
Length bias also impacts the effect of screening programs on overall cancer survival. Length bias identifies indolent or slowly growing tumors that may have a longer pre-symptomatic screen-detectable timeline. Aggressive tumors don't spend much time in the slow growing period therefore detection isn't advanced by routine screening. This contributes to the often misinterpreted "perceived" survival advantage to screen-detected cases. Length bias as described in the graphic may also lead to overdiagnosis--identification of cancers that would not have impacted patient had screening not taken place. 
Like Groundhog Day: the Mammogram Story That Won’t Die
Consider this fact. Cancer cells viewed under a microscope and identifed as cancerous tell us nothing. We are still looking at cells the same way we did 160 years ago--What We Know, What We Don't Know, And What We Believe reveals that we still don't know which cells will be aggressive and which will be indolent. The promise of epigenetics may hold the clue but we do know that just "finding" cancer isn't the key to decreased mortality.
Death rates are improved only where screening has led to a real benefit; they are unchanged where screening has no effect on natural disease progression. 
Here’s the bigger problem: screening mammography has failed to reduce the incidence of metastatic disease and it’s created an epidemic of a precancer called DCIS. The premise of screening is that it can find cancers destined to metastasize when they’re at an early stage so that they can be treated before they turn deadly. If this were the case, then finding and treating cancers at an early stage should reduce the rate at which cancers present at a later, metastatic stage. Unfortunately, that’s not what’s happened.--Like Groundhog Day The Mammogram Story that Won't Die 
Either mammography isn't sensitive enough to identify these cancers early or they don't fit the Halstedian paradigm of steady progression. The lack of change in the incidence of metastatic disease is consistent with the hypothesis that breast cancer is a systemic disease by the time it's detectable — a paradigm typically attributed to Bernard Fisher.--Trends in Metastatic Breast and Prostate Cancer — Lessons in Cancer DynamicsH. Gilbert Welch, M.D., M.P.H., David H. Gorski, M.D., Ph.D., and Peter C. Albertsen, M.D.
If you are a journalist here is a tip sheet from the Association of Healthcare Journalists' website, Advice on communicating the problems with cancer overdiagnosis.Click here for a PDF of the file.
More to come...Improving Numeracy in Medicine (pre-order for only $5.99--price jumps upon publication). Join discussions about how to translate population level risk to individual risk at the patient level (absolute risk). Hint: the inverse of absolute risk is number needed to treat.
Thoughtful discussions about content development and outcomes analytics that apply the principles and frameworks of health policy and economics to persistent and perplexing health and health care problems.
Follow along on Linkedin: here https://www.rebelmouse.com/dataanddonuts/ @graphemeconsult @dataanddonuts @alzheimersbrand
The genesis of an algorithm stems from the desire to break a BIG thing into many little parts. But when we relenquish control to expediency and efficiency we lose the ability to react in real time to what is now relatively automated. Think of Wall Street and the black box that hunts for electronic communications--moving a million shares through the market. Or the last economic crash. Nobody controlled the crash—only the monitor with a red button that said “stop”. We are writing things that we can no longer understand or seperate into components to inform behavior. We lost the sense of what is happening. Unfortunately algorithms are often in conflict with human oversight. Think of the automation strategies of Amazon and Netflix. These algorithms can go out of control and list books like The Making a Fly: The Genetics of Animal Design for $23,698,655.93.
Netflix and Pragmatic Chaos searched for a piece of code 10% more efficient than the current movie recommendation algorithm--and won a cool million in the process. Algorithms are evolving from being a metaphor to actual prophecy. I am thinking that we need to take a few gigantic steps backward. I figure--based on estimates derived on Google and by physician leaders there are literally thousands of guidelines for managing the health of patients. Many of them contradict the status quo and each other, few recommend less care or more deliberate watchful waiting. The Guidelines International Network database currently contains more than 3,700 clinical practice guidelines from 39 countries. Additionally, there are nearly 2,700 guidelines in the National Guidelines Clearinghouse (NGC), part of the Agency for Healthcare Research and Quality (AHRQ). Because of the large number of clinical practice guidelines available, guideline users, including practitioners, find it challenging to determine which guidelines are of high quality. - See more here: Institute of Medicine
On the other extreme, there is an important area of medicine that is still lacking in treatment-based expert review or consensus guidelines. I will write more in another post but I thought it interesting that an important consideration for patients undergoing chemotherapeutic regimens is rarely discussed in public forums.
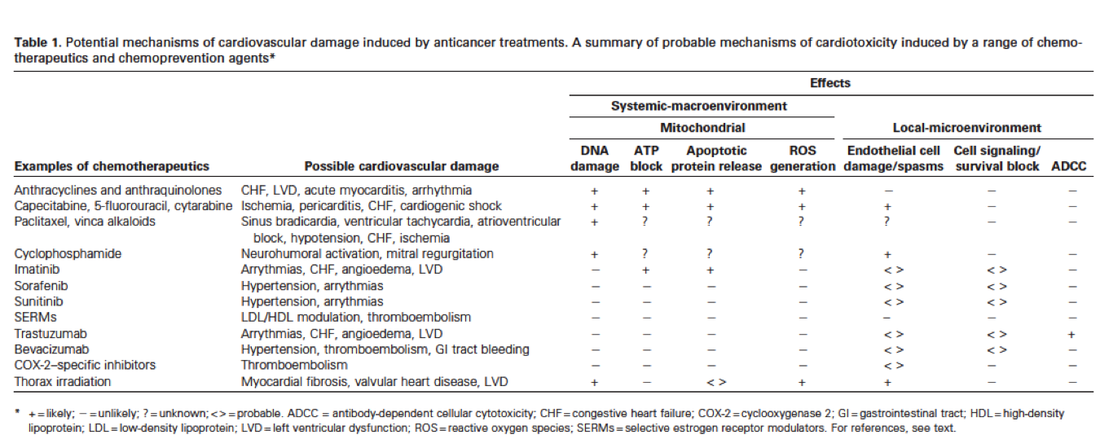
Cardiotoxicity of Anticancer Drugs: The Need for Cardio-Oncology and Cardio-Oncological Prevention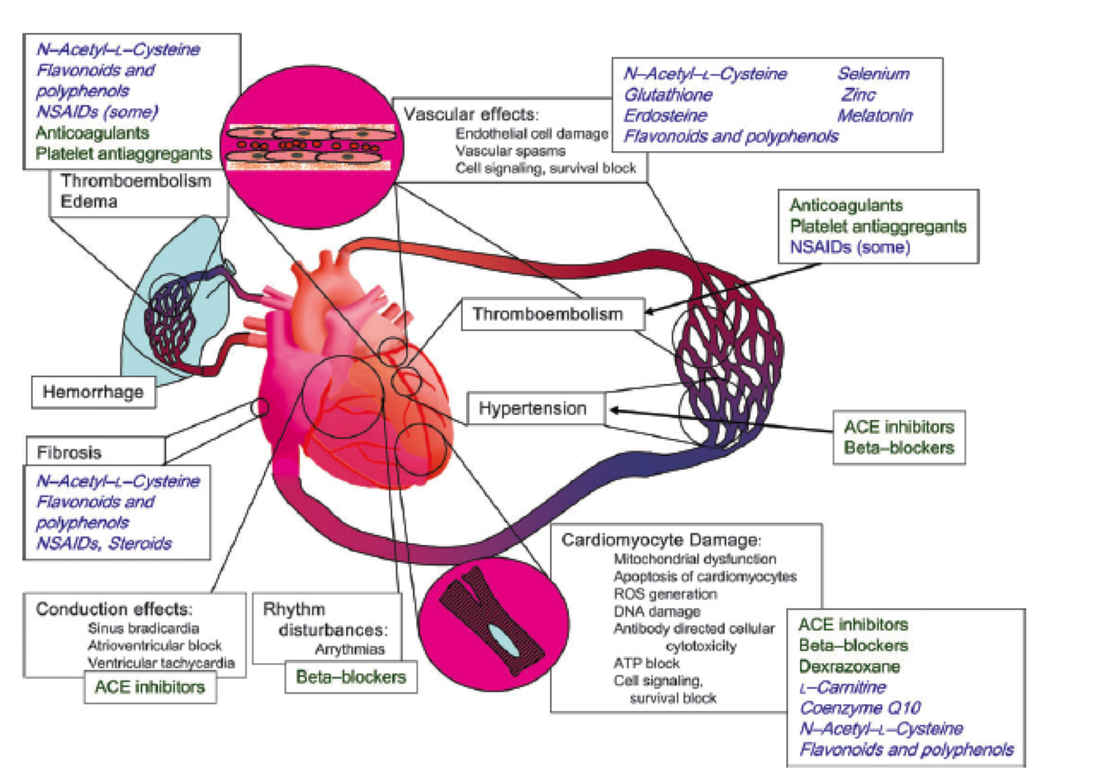
Examples of major mechanisms causing cardiotoxicity of anticancer treatments ( black text ), clinically used therapeutic agents ( green text ),and potential protective agents ( blue cursive text ). ROS = reactive oxygen species; ACE = angiotensin-converting enzyme, NSAIDs = nonsteroidal antiinfl ammatory drugs.--http://jnci.oxfordjournals.org/content/102/1/14.full.pdf+html
Published literature lacks information to guide practioners in the rate of cardiovascular adverse events associated with antineoplastic drugs, particularly for emerging targeted therapies.
In the context of potential overdiagnosis and preventing harms--it is important to understand risks as well as benefits of potentially life-saving at best, or life-altering at worse treatments for cancer amenable to chemotherapy. Quite often the algorithm is in the details--and it is best not to overlook them.
Thoughtful discussions about content development and outcomes analytics that apply the principles and frameworks of health policy and economics to persistent and perplexing health and health care problems.
|

