Have you ever had a doubt about a step along your educational or professional path? Perhaps you omitted data contradicting a client's objective or narrowed your focus so keenly as to obfuscate contrary positions.
I will go first. There was a time when I assumed my role was to write the words I was hired to write. Nothing to see here folks--If the client had a phase III drug about to be approved, the words should plant a fertile field for the industry client to harvest all the spoils. Well, shortly thereafter I realized what I was sowing was carefully edited manure. You could smell it a mile away but what was an independent medical writer to do? I started noticing the data. I was lucky. Numerous stats courses and an ability to learn a little bit of SQL and Python opened many doors to how the data sausage was made. I decided I needed my own platform. Like-minded professionals can gravitate toward or away. As Seth Godin would infer, This is what I made--It might not be for you... Around this time, I attended my first Lown Conference. John Ioannidis presented and my suspicions were confirmed. All was not well in evidence-based medicine. I wrote about his prescient articles numerous times. What follows is a quick summary of what grabbed my attention from Lown 2018--my 3rd Lown conference.
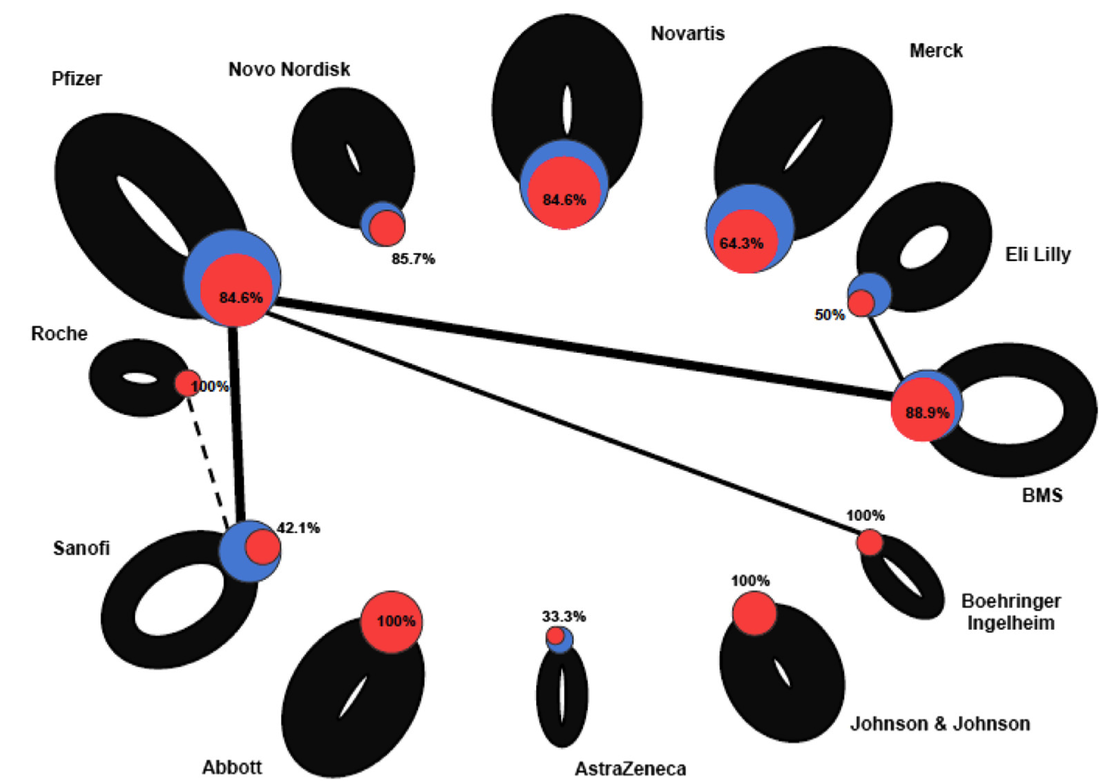
This is the image described in the video. A blue node is a company with the size equivalent to the number of sponsored trials. A link between the node indicates co-sponsored trials. Thin connections or no connections means they didn't test their drug against another drug. The thickness of the line is proportional to companies only investigating its own products or co-sponsored products. The red node indicates favorable results for the clinical trial. This graphic taught me to decipher pharma R&D differently. It isn't about SEC filings--the devil is in the details.
I will be writing more in depth stories about this year's conference. I have a few conversations to distill and a few books to read. First in line is Danielle Martin's Better Now: Six Big Ideas to Improve Health Care for All Canadians. You may recognize Dr Martin from her testimony during senate debate on Affordable Care Act.
Dr. Martin opened the keynote sessions at Lown 2018, How Canada's Successes and Failures Can Inform Our Next System. Canada is single payer Medicare and although it has it's lumps it has lower costs, better outcomes, and does not drive citizens into bankruptcy. She is candid about obvious gaps (no dental, adequate mental health or prescription drug coverage) and reminds us of the cautionary tale of incremental fixes in healthcare.
Powerful discussions from the podium and highlighted in panel sessions emphasize the need for multi-national coalitions to redefine the medical industrial complex for humanity--not profit. A sobering but salient comment, "Prince Edward Island is no match for Pfizer" reminds us that individually--country by country the best efforts will be no match for large power wielding global pharmaceutical companies. Driving what they have branded "innovation" that is in reality, patent protection and share holder investments. In closing, Dr Martin reminded us that Canadian Medicare is narrow but deep--good for what it covers but more is needed. Civic engagement is not about patients but democracy. 
To get a granular look at the current big pharma framework and what a newly minted model might look like I begin with a drawing similar to what I learned here in Business Model Generation: A handbook for visionaries, game changers, and challengers. This is also how I decide what data I am going to need. The upper right quadrant below describes prevention as the main revenue generator with personalized medicine becoming market mainstay--sound familiar?
The colorized image represents the close-up of what that quadrant will look like when we describe key resources and activities, attributes of a competitive value proposition, the role of the customer and their relationships, revenue generation, cost structure re-alignment, and identification of partnerships to maximize drug effectiveness in this new model.
The next few months will be busy working across the lessons learned from the Lancet's series on Canada's global leadership on health. Canada's Universal Health-Care System: Achieving its potential begins the two part series and is a long but worthwhile read. I think I heard correctly that if the US had adopted Canadian prices in the 1960s when US Medicare became law, US workers would have brought home an additional 31 trillion dollars in take home pay to date. I think that is worth investigating.
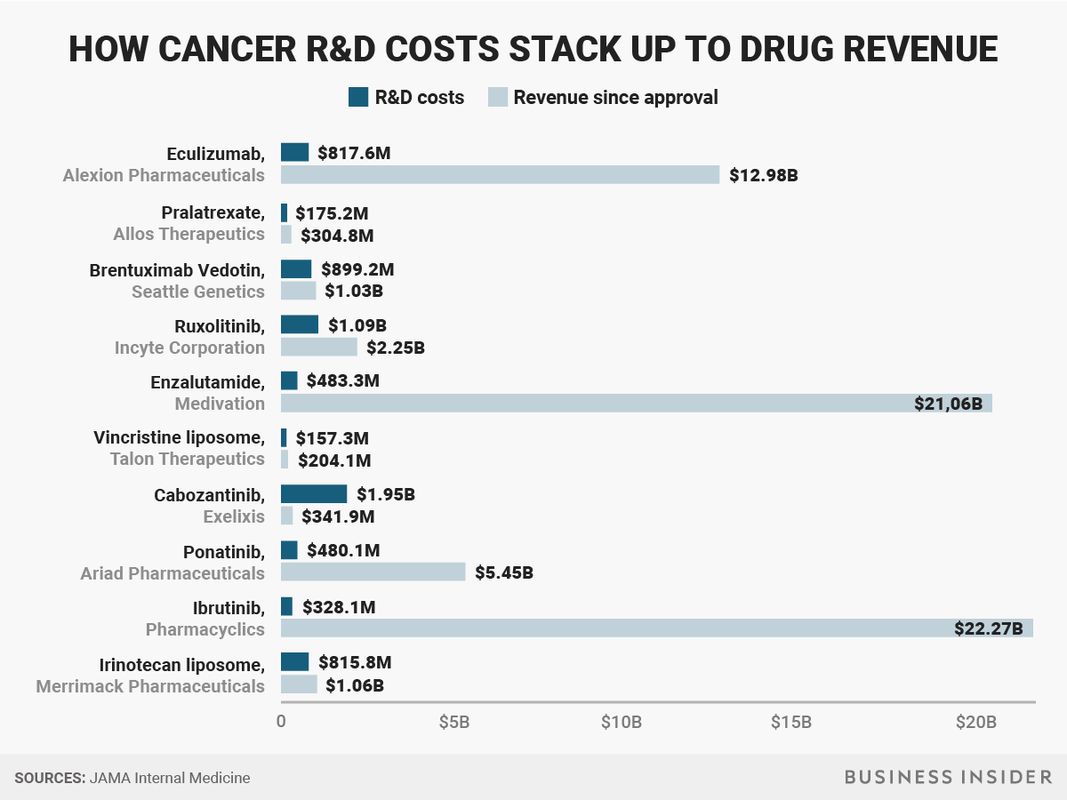
For perspective on what 1 trillion looks like--think of it as time: How Long Ago Is a Trillion Seconds?If you count backward, then: 1 million seconds = 12 days ago 1 billion seconds = 31 years ago 1 trillion seconds = 30,000 B.C. (give or take a decade or two) I am also waiting for Dr. Vinay Prasad's latest article. If you are active in the healthcare sphere on twitter--you likely know Vinay. It should be published soon and a graphic shared at Lown describing false positives in immune-oncology trials and costs and profits associated with randomized controlled trials will continue to illuminate the lagging results in huge oncology pipelines. 
Dr. Prasad's work has demonstrated that many medical practices, promoted and advocated for decades, are ultimately shown not to work. These reversals typically occur when we adopt new therapies based on incomplete or inadequate studies. Dr. Prasad has also demonstrated that the high cost of cancer drugs is not explained by rational factors, that media coverage of medical articles preferentially covers lower levels of evidence, that industry sponsored randomized trials have substantial bias, and that many current medical practices have no convincing proof of efficacy (e.g. IVC filters).
Follow along here or on twitter or instagram...If any of the words resonate in any way please feel free to buy me a coffee or two. It helps fund the travel and the research.
Thank you again to my sustaining donors! I could not do it without you.  Think about the amount of investment in R&D for cancer. The 21st Century Cures Act authorized $1.8 billion in funding over 7 years. Much of the research earmarked for the upstream social determinants of health and prevention was diverted. What is our societal return on investment? Insights are driven from the margins. Those of us merging different industry perspectives are loaded with questions. The US National Cancer Institute (NCI) bet on these evolving questions when inviting physical scientists to join the debate identifying novel approaches to cancer etiology. What if cancer tumors are indeed atavisms as speculated by Paul Davies? Introductory courses on embryology mention pharyngeal gill slits, rudimentary tails and other remnants of aquatic life. In the majority of instances these genes are silenced as development progresses but ancestral traits sometimes remain--these are called atavisms. As a physicist and director of the Beyond Center for Fundamental Concepts in Science at Arizona State University, Dr. Davies suggests a theory that a disruption in silencing ancestral genes allows cancer to activate an "ancestral core" that mirrors evolution but in reverse--conferring malignant traits.
But challenging the status quo isn't for the faint of heart. Somatic mutation theories describe the random and unpredictable nature of genetic mutations but what if we can appreciate the deceptively organized behavior of cancer across a wide variety of tissue types? Collaborations crumble when pre-ordained objectives don't hold up to intense scrutiny or verification in external databases. I was surprised how many executives and self-prescribed experts lack curiosity. I worked with a team that requested data from a pharmaceutical client's investigator's brochure--but none of the relevant content. Understanding why a client is launching a second or third to market oncology drug is vital information. Assumptions made in the pre-clinical phase of drug development matter. An article by a physicist and an oncologist, Stochasticity and Determinism in Cancer Creation and Progression should bring about a lively debate. Think of stochasticity as randomness and determinism as an assumption that the predictability of genes alone can explain a theoretical construct. Does the cancer subroutine possess a genomic fingerprint? In addressing the question of genomic changes in cancer, it is crucial to distinguish between mutations, where gene sequences change, and gene expression, where sequences are unchanged but normally silenced genes become switched on (or vice versa). I think we all try to do better. Unfortunately our Google searching brains neglect to appreciate that granularity rarely floats to the top. The easy data to access is rarely the right data. Most descriptions of cancer progression focus on the proliferative aspect. It is well known that the tumor burden per se can usually be successfully reduced by a variety of clinical interventions—surgery, radiation and drugs—but that for metastatic cancer this approach rarely eliminates the disease completely on account of the phenotypic changes resulting in advancing malignancy. By concentrating on gain-of-function properties, such as the aforesaid proliferation, therapeutic strategies typically target cancer's strengths. But by defaulting to an ancestral phenotype, cancer cells lose more recently evolved functionality. This loss of function may represent the Achilles' heel of cancer, and therapies designed to target cancer's weaknesses may offer a more hopeful and unique alternative for the future I am reminded by the words of a brilliant poet, David Whyte. The full poem is at the link. Coleman's Bed "...Live in this place as you were meant to and then, surprised by your abilities, become the ancestor of it all, the quiet, robust and blessed Saint that your future happiness will always remember." Here he reflects on the poem edited from Oprah's-Lifeclass.
Are you thinking differently?
 My brain hurts. Have you ever been hired as a data analyst or writer and realized perhaps the "truth" wasn't the actual requested deliverable? Maybe there are truthier truths and they are available on a sliding scale based on what pleases the client. I don't mean to be harsh but most of us have seen certain data sources preferentially requested when opposing views are found in the curated findings. Headlines often misrepresent the risks and benefits of novel therapies to the general public and clinical researchers as well. It is not a surprise--or it shouldn't be--that there is confusion at the point of care. Kite’s treatment, a form of immunotherapy called CAR-T, was initially developed by a team of researchers at the National Cancer Institute, led by a longtime friend and mentor of Dr. Belldegrun. Now Kite pays several million a year to the government to support continuing research dedicated to the company’s efforts. The relationship puts American taxpayers squarely in the middle of one of the hottest new drug markets. It also raises a question: Are taxpayers getting a good deal? “Enthusiasm for cancer immunotherapy is soaring, and so is Arie Belldegrun’s fortune.” Promising oncology drugs classified as immunotherapy are creating an effective platform for demanding top dollar. These debates all have the same framework. Research & Development costs soaring (even though M&A is hot hot hot), risky to bring drugs to market, innovation will dry up without scary pricing and looming financial profit, and a host of other reasons the market should decide who will be able to access potentially curative therapies. These are not simple tensions to resolve. What about transparency? If we are going to continue the "market" debate for pricing then we need to bring more aspects of a free market to bear. Overlooking the obvious violation of free markets (patients don't voluntarily become sick) there is a lot we don't know about the cost of producing clinical grade cellular therapies. Estimates are pretty low and vary around $14000 to $16000 per patient. But production appears to be the smallest influencer. There are supplies, QC testing, services of trained technicians, facility costs and more granular line items not described for public consumption or understanding.
 The Bayh-Dole Act introduced a set of guidelines for all federal funding agencies to grant ownership of innovations to the universities and researchers that developed them. Now license terms were able to be freely negotiated leading to more ideas and economic growth. Seemingly a successful piece of legislation, Bayh-Dole secures intellectual property rights allowing commercialization of federally funded research. There has been discussion of citing the "march in" provision of the act. You may be familiar with a petition backed by Senator Bernie Sanders to allow the government to control escalating drug costs by citing the march in provision of the Bayh-Dole Act. March-in rights give the federal government the right to grant other entities licenses or even to themselves if they gained funding for the patent. The wording is being debated. Should march-in rights consider high drug costs as a threat to public safety? There are critics of a less restrictive patenting and technology transfer. The outcome--as some believe--promoted excess granting of patents and created restrictive licensing. I suggest reading the opinion rendered in Association for Molecular Pathology v. Myriad Genetics about the claim of ownership of BRCA1 and BRCA2 genes--Patents, Profits, and the American People — The Bayh–Dole Act of 1980 When the Bayh–Dole Act was written, its aim was primarily to stimulate economic growth by more efficiently mining the untapped scientific riches of hospitals, laboratories, and universities. Much has changed since then. Hard to argue that our present biotech landscape was considered back in the 1980s. How are we defining "public benefit"? Does the public as a whole benefit or are the benefits and profits funneled to a few at tax payer expense? The Bayh-Dole Act of 1980 mandates that universities take on the responsibility to transfer the novel technologies that arise from federally sponsored research. The objectives are to introduce new products in the market for public benefit and to enhance entrepreneurship--Patent and License Pearls and Pitfalls for Taking an Idea to the Marketplace I recommend the interactive calculator below for looking at value metrics around drug pricing. How much should cancer drugs cost? described the tool but the methodology is insightful as we decide how to price emerging investigational products. The Drug Pricing Lab includes the following domains allowing modifiable price components selected by user--efficacy, tolerability, novelty, research & development costs, rarity, population burden, unmet need, and prognosis.  Profits and patents can be powerful incentives for scientists, businesspeople, and universities, but new and ongoing risks — including high prices that limit access to lifesaving technologies, reduced sharing of scientific data, marked shifts of focus from basic to applied research, and conflicts of interests for doctors and academic medical centers — should be mitigated or averted through revisions of the law. All Americans should be able to share in the bounties of federally funded biomedical research.--Howard Markel, MD, PhD, NEJM 2013  We are at capacity for the San Francisco venue but don't miss the all female roundtable on Facebook Live. The Future of Pharma: Getting Sh*t Done (GSD)
 Most days I feel like the luckiest person alive. I get to travel as much or as little as I desire and along the way I meet the leading minds in healthcare, health policy, and even economic theory. You know what they say about being the smartest person in a room? Find another room. But it isn't without challenges. Headlines herald new breakthroughs and advances especially in oncology--but the data is actually distorted to skew towards a cure rather than a potential stepping stone. For example, when I read the statistics sections of clinical research reports I see the interchangeable use of multivariate and multivariable analysis. To begin to see light between these two terms, we need to understand the difference between a categorical and a continuous variable. Here is an excerpt from a small book I wrote as a guide, Improving Numeracy in Medicine.  You have heard of regression models. Outcome variables in linear regression models are continuous while logistic regression variables are categorical or have a binary outcome--survival analysis is time to event. Multivariate analysis in a sense is referring to statistical models with 2 or more dependent or outcome variables. Multivariable analysis refer to multiple independent or response variables. A simple linear regression model will have a continuous outcome and one predictor while multivariable linear regression models have a continuous outcome and multiple predictors (continuous or categorical). Whats the big deal? Maybe there isn't one. Remember I am not a statistician but when I see the wrong model being used or described in the methods or results section I begin to arch my eyebrow and try and unpack the mathematics. After all, the articles are written for informed decisions and often--important interpretation at the point of care. Data is like a living organism. Depending on when you collect or how you collect the data you may only be capturing a "moment in time" and nothing more. We need to be more cognizant of making informed decisions at the intersection of multiple data sources and perspectives. Methods used to generate the data should be transparent and reproducible. I keep this series on Evaluation of Scientific Publications handy--Survival Analysis.  As a professional reviewer I often see the mishmash of terms and confusing model selection. Remembering the dynamic nature of the data we collect may go a long way in seeking robust statistics and open dialogue around what we can and can not infer...
"Statistics are like swimwear - what they reveal is suggestive but what they conceal is vital."9/19/2017
The quote is part of my email signature. It reminds me of the complexity of decisions being made at the point of care by both healthcare providers and patients. "Patients have unprecedented access to health information, but lack the skills to interpret it", says Dr. Mahajan. I would argue that healthcare providers are in the same boat. I often query statisticians at conferences such as the Joint Statistical Meetings--"Who is the intended audience for your models and debates?" At times it seems like complex numeracy is left for those of us perhaps with a high degree of numeracy but often not linked to ideologic debates of statistical context. A big data challenge in consultancy is having to tell a client their "baby is ugly". Data frameworks are created during pre-clinical planning and brand teams often aren't aware of the role they play in positioning or eventual marketing of an intervention or therapeutic. Discussing the limits of the wide-eyed optimism often rampant in drug discovery does not make you a popular member of the discussion. But I would argue, perhaps one of the most valuable. Full disclosure, these are a few of the graphics I have recently used while discussing these topics with groups either bringing a drug to market, understanding the competitive landscape, or guiding stakeholders through what gets reported and what it actually means to their individual perspectives. Links are included for additional granularity. One of the retained channels of direct physician communication remains continued medical education or CME. I continue to argue many are wasting the opportunity by relying on self-serving myopic educational offerings while simultaneously limiting data collection and analyses to the "been there, done that" mentality of whatever hegemonic framework they are promoting (monetizing). The journey to "value-based" care is paved with vague terms like "value" and "innovation". Patients, industry, FDA, and insurance companies for example all have unique tensions around bringing innovative and effective therapies or interventions to patients as quickly as possible. Oncology, in recent months has been the poster child of "hurry up and wait". Trials are trying to move faster with smaller patient populations often identified by pre-determined markers of success dependent on a heterogeneous group of clinical trial endpoints. How do we sift through the data and clinical findings? 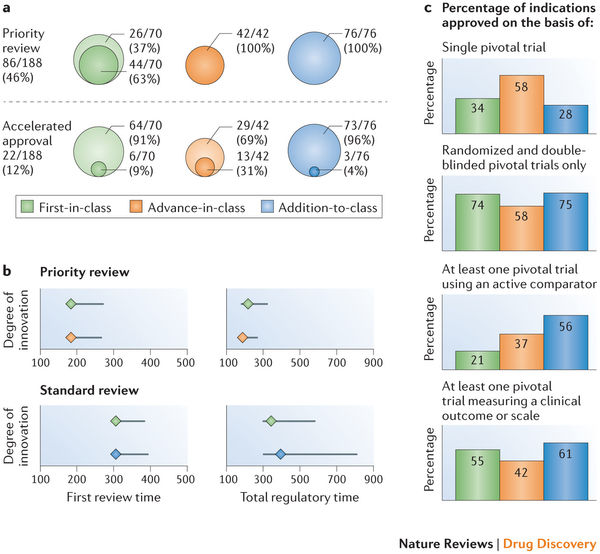 A compelling argument can be made for developing a framework to validate surrogate endpoints. ...surrogates can result in market access for technologies that turn out to offer no true health benefit — or even cause harm —and can result in overestimation of treatment effects (and economic value), which can lead to inappropriate decisions on coverage. Use of surrogate end points in healthcare policy: a proposal for adoption of a validation framework--Ciani, Buyse, Drummond, Rasi, Saad, and Taylor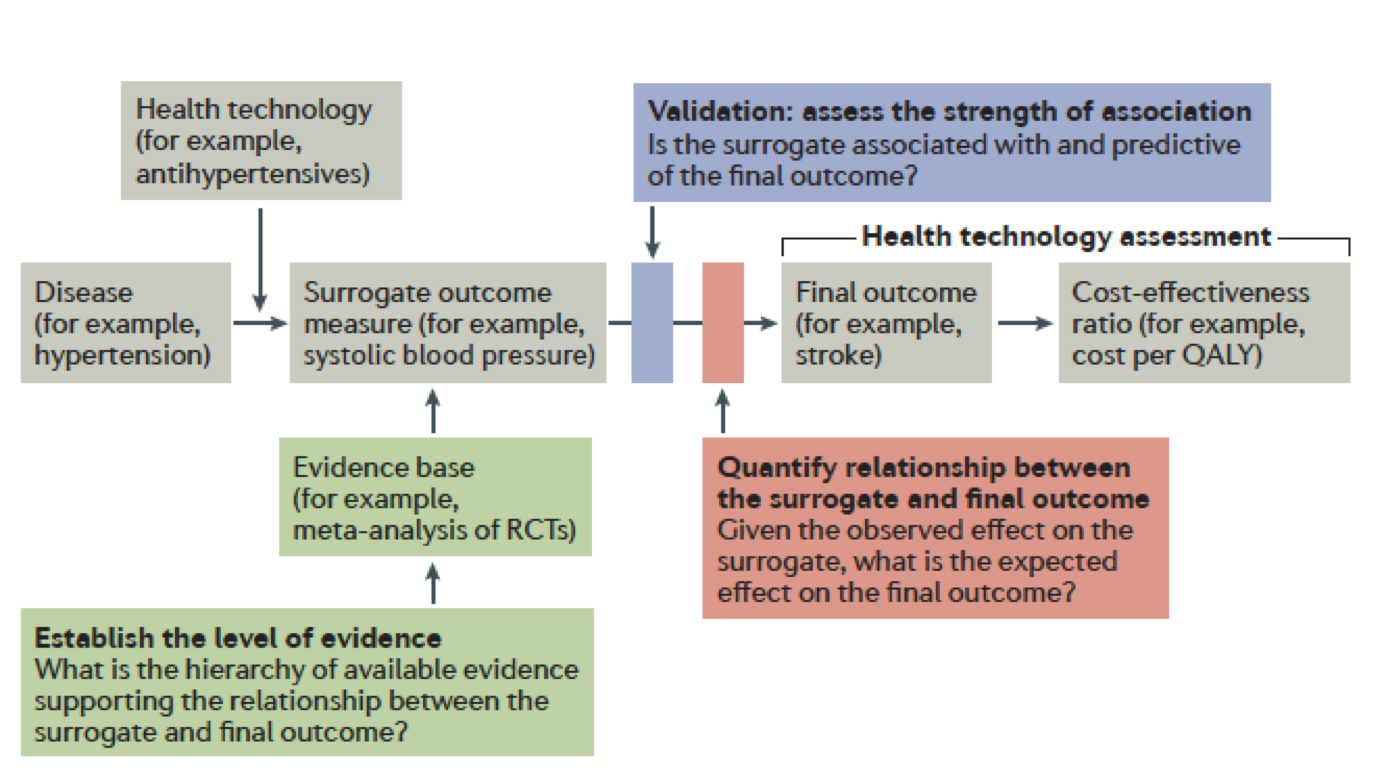 You should be left with questions. Lots of questions. •Can absolute standards of surrogacy be defined? •Is association approach sufficient or should surrogacy be further explored using causal inference? •If a surrogate is valid for a specific treatment, is it still valid for other treatments? •Is constancy assumption reasonable (changing treatment landscape)? •Can incomplete surrogate be used e.g. for rescue therapy? The Surrogate Threshold Effect (STE) for EFS as potential surrogate for OS in patients treated for Acute Myeloid Leukemia (AML)--Buyse, Schlenk, Donner, Burzykowski-- JSM 2017  Here is the hot tip for improving critical thought and analytic approaches. First, it matters because the quality of debate and consideration prior to late-stage clinical trials or drug approvals--the better the outcomes for all stakeholders. Public workshops are the best training ground for improving expertise in the validity or weakness in certain data/statistical models. A recent in-person session of Duke-Margolis Center for Health Policy titled Public Workshop: Scientific and Regulatory Considerations for the Analytical Validation of Assays Used in the Qualification of Biomarkers in Biological Matrices focused on discussion of this white paper.
We all have those annoying little quirks that left unchecked can drive us mad. I always look at objectives. The big data projects have them, clinical trials have them (endpoints), medical education, research articles (null hypothesis), they are every where. My stone in the shoe is how poorly formed and ill-defined they are. Regardless of what we call them, often they are not actionable, measurable, temporal or in the case of clinical trials--relevant. Let me explain.
It seems that precise and well defined objectives carefully placed on a path to robust discoveries may be self-limiting. What if the most innovative discoveries aren't waiting to be predicted in advance? I would argue that maybe we need to identify the steps along the way--not knowing where they might lead. For example, perhaps there are populations of cell types or immuno-signatures potentially missed if we don't redefine what success looks like along the way to a singular objective--improving overall survival for example.
If Deep Learning focuses on programming an artificial neural network (ANN) to learn, Neuroevolution focuses on the origin of the overall architecture. We learn about artificial intelligence by comparing it to how the brain works. Our network connections simulate the neurons of the brain. ANN simulates these connections with stronger connections having more nodes or "weight".
What does it mean to make progress in neuroevolution? In general, it involves recognizing a limitation on the complexity of the ANNs that can evolve and then introducing an approach to overcoming that limitation. For example, the fixed-topology algorithms of the '80s and '90s exhibit one glaring limitation that clearly diverges from nature: the ANNs they evolve can never become larger.
If this area interests you or you are working in machine learning and large datasets read about a new class of algorithms called "Illumination algorithms" a modern approach to neuroevolution. The shift is to focus on a broad cross-section of workable variations of what might be possible instead of looking for a single "optimal" solution.
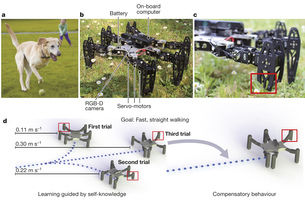
The main reason for integrating neuroevolution into the discussion has to do with the latest advancements in immuno-oncology. If we think of recent phase III failures--perhaps we are too focused on objectives or clinical study endpoints such as overall survival and progression free survival. Defining a broad cross-section of workable variations might be more successful and informative.
Chimeric antigen receptor (CAR)-T cell infusion has demonstrated an increase of many genes in predefined immune signatures, including t-cell related genes, chemokines, checkpoint inhibitors, and lymphocyte-activation protein 3 (LAG3). Maybe there are too many clinical steps along the path for a singularly-defined objective to serve research goals or more importantly--patients. For example, wouldn't it be informative to address the complexity of cancer as a system? We have multiple measures rolled into a clinical trial endpoint that decides whether a investigational product progresses to the next phase, what patient may benefit, and who funds the research. Meanwhile we must consider pre-existing immunity, type and density of immune cells, spatiotemporal dynamics of intratumoral immune cells, cancer vaccines, the role of cytokines, CD122, T cell bispecifics, and a host of other immune factors. Bringing to Life the Science around Innovative New Drugs, Gene and Cell Therapies--noveltargets.com
A straight path never leads anywhere except to the objective.--Andre Gide 
Darwin's theory of evolution is a framework by which we understand the diversity of life on Earth. But there is no equation sitting there in Darwin's 'Origin of Species' that you apply and say, 'What is this species going to look like in 100 years or 1,000 years?' Biology isn't there yet with that kind of predictive precision.--Neil deGrasse Tyson
Our precise understanding of the complex biology behind cancer immuno-oncology lags the reported outcomes observed in clinical research. Case in point--the best therapies on average confirm clinical trial endpoints in approximately 20 to 30 percent of patient populations. I would argue that we are measuring the wrong thing but more about that later.
In the last 6 months to a year I have been working almost exclusively in the immuno-oncology space. Either directly with industry, on a collaborative team, or as a numeracy expert helping physician groups and/or patient advocacy groups unpack the latest findings. After attending the World Vaccine Congress, Immunology 2017, DIA/FDA Statistics Forum, and Duke-Margolis Center for Health Policy/FDA workshop on analytical validation of assays used in qualifications of biomarkers I can tell you the headlines announcing potential cures and breakthrough approvals for checkpoint inhibitors are misleading and superficial in their conveyed messages. Here is a simplistic representation of immunotherapy to introduce you to the basic premise in case this isn't an area of expertise.
The Cure in the Code: How 20th Century Law is Undermining 21st Century Medicine by Peter W. Huber describes the historical precedence and evolving shift of a small molecule mind-set to the rise of biomedical science and the power of a data-enabled framework. The first-pill costs are markedly more expensive than the later-pill costs--the true excipient is the "know-how". Are we ready to rethink our mindset? How do we market knowledge?
What if we approved drugs based on the biochemistry. Similar to Eureresist what if drugs were classified based on their ability to increase trafficking and penetration of tumor by T cells, T cell activation, and quantity of tumor-specific T cells for example. We can look at the graphic and see the myriad of options. What may result is the combination of HIV style cocktails that tailor treatment to the specific biochemistry of the tumor AND the patient. In the absence of clunky monotherapy or combination therapies we don't truly understand--we now have measurable endpoints beyond overall survival, progression free survival, etc. 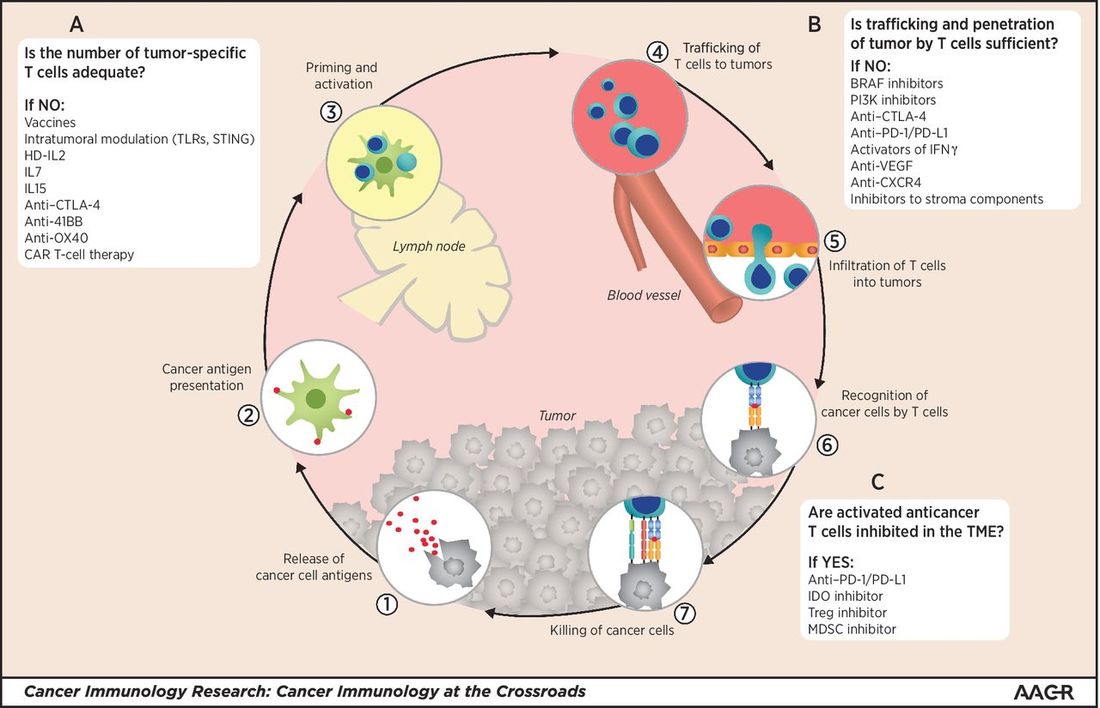
Why is the latest data from Keytruda heralded as the success of ASCO while Opdivo, once the industry leader is losing it's footing with less than impressive two-year survival update on its Opdivo-Yervoy first-line lung cancer? I am going to point to the complexity of identifying appropriate biomarkers.
The most-effective to date has been PD-L1 expression but we shouldn't be convinced of a simplistic one biomarker gateway. An article published in 2016 by Manson and colleagues Biomarkers associated with checkpoint inhibitors highlight biomarkers with the potential to predict efficacy and toxicity. 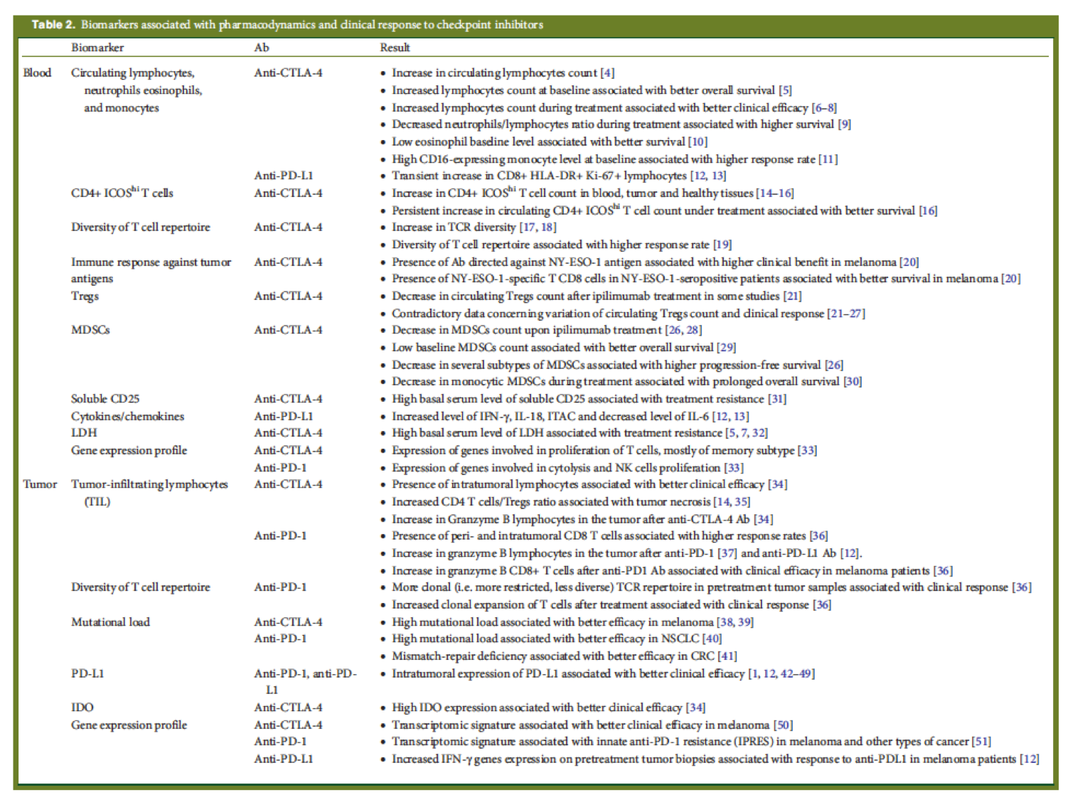
The Biomarker Assay Collaborative Evidentiary Considerations Writing Group, Critical Path Institute (C-Path) includes scientists from the FDA, industry and academia collaborating to establish scientific and regulatory validation of biomarker assays. The process is ongoing and complex and includes a "framework" approach vs. a "checklist" to help stakeholders quantify and validate their assays effectively.
Inherent in the measurement of biomarkers, unlike the measurement of xenobiotics (drugs), is that biomarkers are endogenous entities or molecules. Therefore, biomarker assays typically measure an increase or decrease in the endogenous level of the molecule which often fluctuates because of individual variability in physiology, disease biology, pathology, comorbidities, treatment administered, and environmental factors. Given these factors, the requirements and expectations for assays used in the qualification of biomarkers must take into consideration 1) the type of molecules being measured and 2) the context in which the biomarker is being applied in drug development and in regulatory decision-making.--Public Workshop Duke Margolis Center for Health Policy, DC 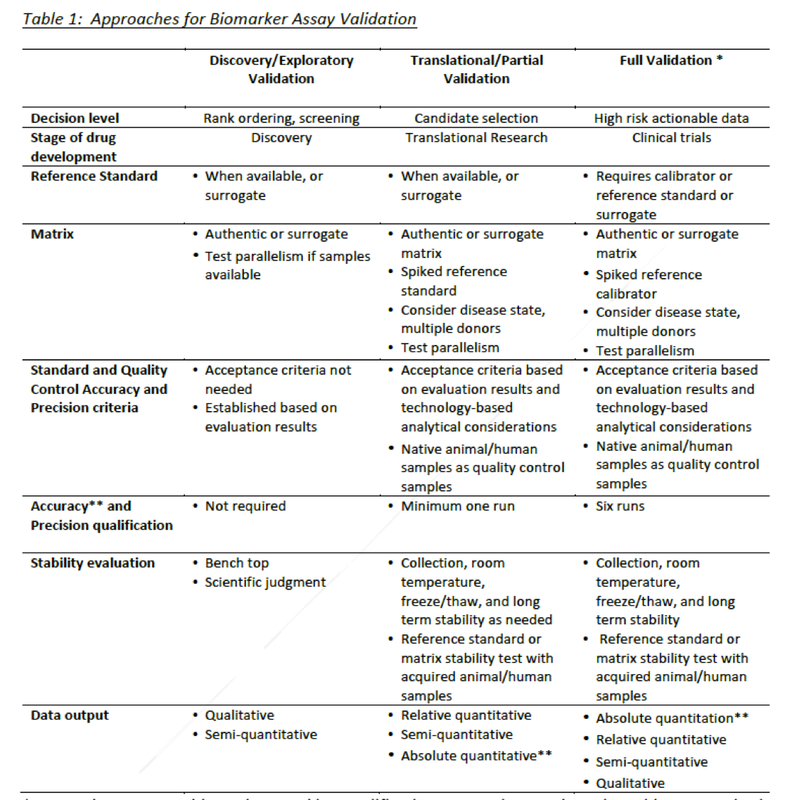
The new prescription for medicine might indeed be ex uno plura--out of one, many--an evolution from epidemiology and crowd-sourced aggregated solutions to single-gene perspectives and truly tailored treatment for the unique biochemistry of an individual.
There is a lot of crowd speak about reforming how we develop drugs--especially in the US. Don't get me wrong, I listened carefully during the DIA/FDA Statistics Forum about adaptive frameworks, pragmatic trials, how to analyze real world evidence and integrate findings with clinical trial data generated from well-defined, perhaps ineffectual, clinical endpoints. There also seems to be an inexhaustible variety of innovative strategies being circulated to manage the ginormous data deluge and focus on patient driven outcomes. As a writer coming of age both personally and professionally during the early years of the HIV crisis I remain curious about our relative amnesia or short attention spans for the hard-won lessons learned during a pivotal time in clinical science. The most powerful patient advocacy in the world drove the positive outcomes and clinical successes most of us take for granted. The leading edge of the science existed at the front line--well before long-term outcomes in efficacy and safety were established. I don't want to ruin your morning but dear reader, "safety" is not even a scientific term. Because of the "interesting" evolution of the Food And Drug Administration (FDA)--and you definitely should read up on how we landed where we are today--and how gaps persist where real science can occur (The Cure in The Code: How 20th Century Law is Undermining 21st Century Medicine)--we are forgetting, at our own detriment, how off-label prescribing, critical thinking, and physician/clinical scientist group-think led to Euresist. The development of an international computer-based clinical management of antiretroviral drug resistance informed providers about what to do if a patient's viral load--once suppressed--escalated. What therapy or cocktail has proven effective?
The physicians were prescribing drugs effective in leprosy to patients with aggressive fungal disorders, wasting syndromes, and oral and genital canker sores characteristic of AIDS--not because they were FDA approved--but because they worked. The evolution of EuResist provided a tool for physicians to make evidence-based decisions (even if evidence was still evolving at the clinical level) at the point of care outside the government process that had proven to cumbersome to respond to the scale of morbidity and mortality. EuResist Network is a partnership of eighteen institutions in Europe and beyond, which promotes and coordinates joint research and dissemination efforts of its partners. As my inbox "pings" with late breaking news of ASCO data and invitations to webcasts I think we are witnessing the pivot from compassion and improving patient outcomes to expanding market share and market driven profits. I am not tossing babies out with volumes of bathwater--but seriously--where is the framework for a free open-sourced group think? I know there are pockets of sharing. I have written about them here. The model of for-profit data outpaces the network open-source solutions. Huge databases are amassed with partnerships boasting genetic libraries, claims data, clinical trial data and real world data--for a fee. A whopping fee with no promise of relevance or operational insights. What is the solution? Provide context and conceptual understanding so healthcare providers can group-think knowing they have actionable data. An ever increasing number of immune-oncology (I/O) therapies are being granted break-through designations. I am excited to hear the latest data from larotrectinib, a novel selective TRK tyrosine kinase inhibitor (TKI). The high response rate is intriguing. Those of us lucky enough to be present in science have a responsibility. Not to repeat sensationalized headlines but to help unpack the data in an industry agnostic manner. What do findings mean? Real world data is generated one patient at a time. It is up to us to assess real world evidence and share the narrative. It will be the providers at the point of care evaluating tumor genetics, micro-environments, mutational attributes of exomes, neoantigens, cell-cell signals of kinase pathways, and more as 'n of 1' findings outnumber epidemiological population estimations. Despite durable responses to TRK kinase-directed therapy in patients with NTRK-rearranged A sentence in The Cure in the Code has stayed with me, "A drug can be judged unfit for the market, one arm of government limits what the drug company may say while another invites juries to read lies or broken promises into its silence-Peter Huber
Stay-tuned for findings from the LOXO webcast scheduled June 4th...
There is a lot to unpack regarding the latest science around immune-oncology and the dizzying pace of breakthrough approvals for checkpoint inhibitors and emerging science addressing personalized medicine. Basically, the outcomes have outpaced our understanding of the biology--but the forum of the World Vaccine Congress certainly softens the learning curve. Jessica Fletcher, PhD from Genocea, a "vaccine company" shared an informative slide on the correlation of mutation profile to objective response rate (ORR), the proportion of patients with reduction in tumor burden of a predefined amount, to checkpoint blockade therapy. As depicted on the graphic below, mutation mismatch repair deficient (MMR-D) colorectal cancers (CRCs) have a more favorable stage-adjusted prognosis or outcome compared with MMR-proficient tumors (MMR-P). Not to over-simplify, but the more non-self an antigen, the more likely it is to elicit an immune response.  The Cancer Genome Atlas (TCGA) data portal contains harmonized cancer datasets within the National Cancer Institute Data Portal. This is an important resource for data projects within oncology reliant on genomic data. As a big believer in transparency and accessibility, I only share data sources that are either free or have minimal fees for access. I can answer specific questions on how to access this data or perform advanced search queries but what follows here are illustrative examples to highlight the complexity of mutational landscapes. Mutational landscape and significance across 12 major cancer types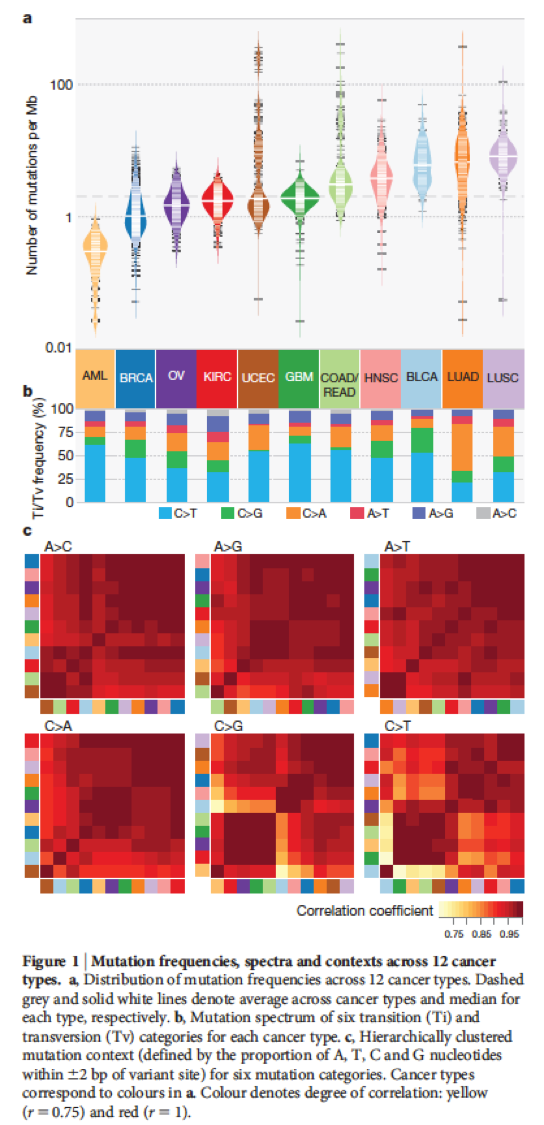 Somatic variants from 3,281 tumors across 12 tumor types from the TCGA Pan-Cancer analysis highlight "distributions of mutation frequencies, types and contexts across tumor types, and establish their links to tissues of origin, environmental/carcinogen influences, and DNA repair defects". What is important to observe is the sheer volume of mutations accumulated within human cancers with the majority being unique to individual patients. Below it is apparent that only a small percentage of these mutations are mutagenic. 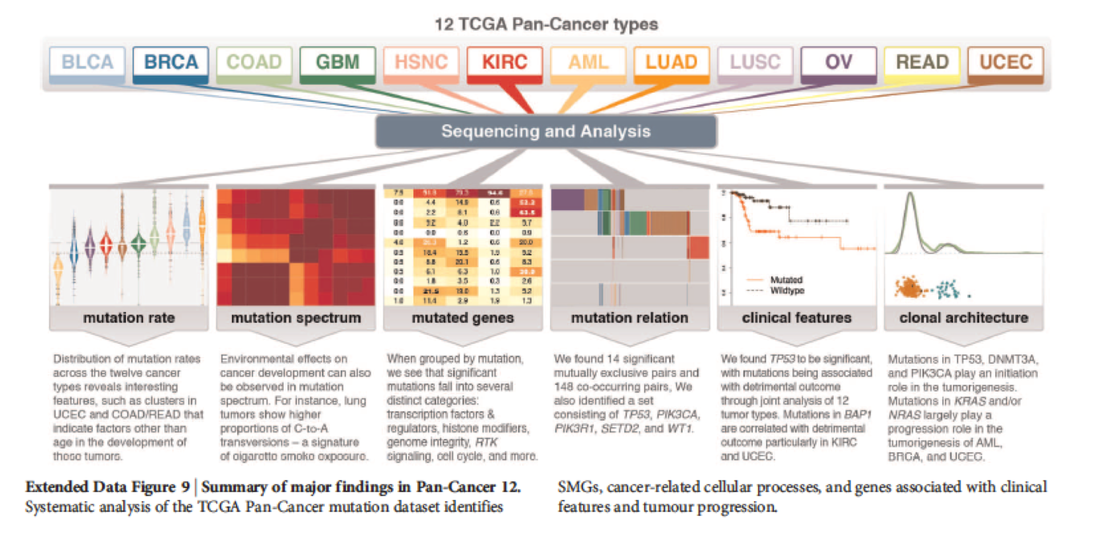 It begs the question regarding broad epidemiological frameworks applied to genetically unique clinical outcomes. Outcome measures and clinical trial endpoint selection are hotly debated as they are inconsistently applied across immune-oncology trials. A convenient chart published in Oncology Endpoints in a Changing Landscape is an informative introduction to surrogate endpoints used in clinical research when overall survival isn't feasible. 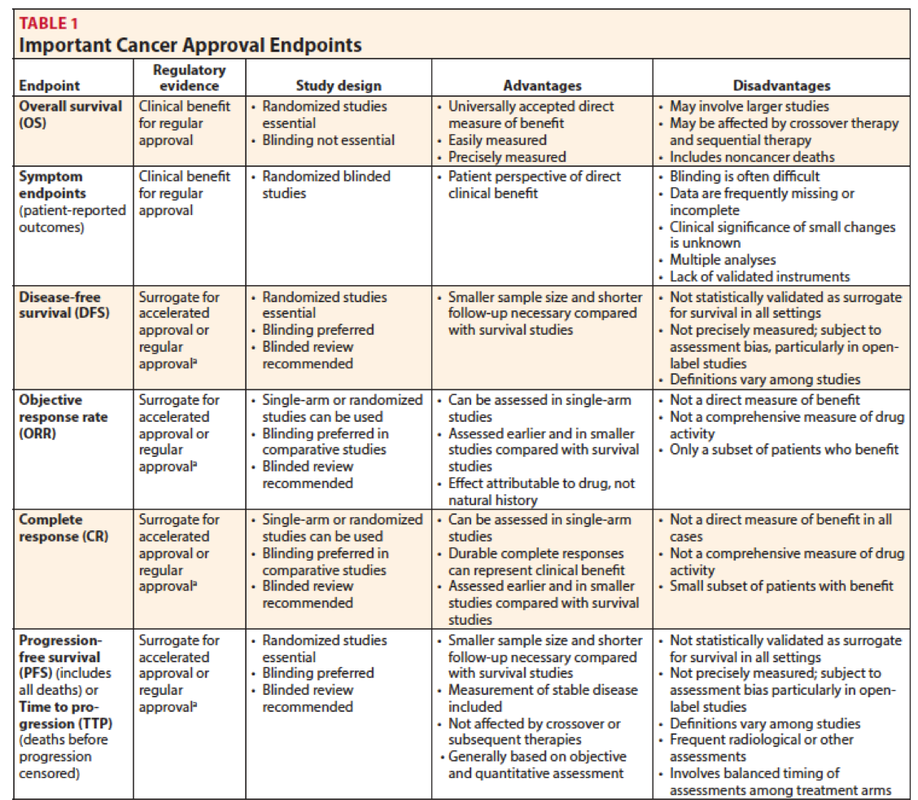 There is much to learn, discuss, and discover in the evolution of our understanding of immune-oncology. Join the discussion or read along--stay-tuned... Epidemiological, genetic and molecular biological studies have collectively provided us with a rich source of data that underpins our current understanding of the aetiology and molecular pathogenesis of cancer. But this perspective focuses on proximate mechanisms, and does not provide an adequate explanation for the prevalence of tumours and cancer in animal species or what seems to be the striking vulnerability of Homo sapiens. The central precept of Darwinian medicine is that vulnerability to cancer, and other major diseases, arises at least in part as a consequence of the 'design' limitations, compromises and trade-offs that characterize evolutionary processes.--Mel Greaves, Darwinian medicine: a case for cancer  What a fantastic time to be in the world of scientific discovery. I have been at the bench, in the halls of academia (as a student and medical writer), worked in industry, employed as a medical education executive, and most recently, I work as a datapreneur. What is that? I like to describe datapreneur as a journalist taking cues only from data. Discovery in the sciences is dynamic. Regardless of your pedigree or educational attainment, if you aren't in lockstep with advances in your chosen discipline, you are obsolete. There is texture in experience. And insights to gain from tireless scientists hoping to advance if not a cure perhaps a better quality of life during advanced and chronic cancers.
|